Original research
By Pompilio Martinez, MD
Alumnus, School of Medicine, National University of Colombia
Ex-investigator, Colombian National Institute of Health, Bogota, Colombia
Abstract
Here I describe neurological symptoms of 62 girls who were immunized against the human papilloma virus (HPV). Most participants (61) are Colombian and received the quadrivalent HPV vaccine Gardasil and a girl from Mexico received the bivalent Cervarix vaccine. The average age was 14.5 years (SD 2.1). This survey reveals an overall pattern of peripheral nervous system damage as demonstrated by complaints of inflammatory and neuropathic pain syndromes in the head, back, chest, arms and legs. There were also sensory and motor syndromes with upper and lower limb numbness and tingling (paraesthesia), muscle weakness and difficulty walking (paresis) accompanied by tremors, muscle spasms and twitches (abnormal movements). Most symptoms appeared after the second vaccine dose, which agrees with greater antibody titers seen in booster dose immunizations. – A severely ill 13-year old girl with similar complaints and history of immunization, had high serum auto-antibody titers against nerve tissue as well as marked clinical improvement after anti-inflammatory and antibody removal therapy (plasmapheresis and IVIg). This evidence prompts me to propose an autoimmune hypersensitivity type II reaction triggered by Gardasil whose batch-specific antigens await further research. The general disease pattern described here is consistent with a demyelinating disorder that might not apply to every girl therefore every one of them should be diagnosed and treated individually. This humble survey hopes to uncover leads to help the investigation sought by the Colombian Higher Courts. We must acknowledge the role played by Health Minister Alejandro Gaviria whose indiscriminate massive immunization campaign as well as absolute neglect and outward mishandling of the epidemic of Serious Adverse Events makes him worthy of consideration for the Nobel Prize in the category of Crimes against Humanity. We hope the International Criminal Court takes action on this issue, today a global matter. We invite scientists worldwide to investigate HPV vaccine lots to understand this disease.
Por favor lee la versión en español o castellano de este artículo.
Introduction
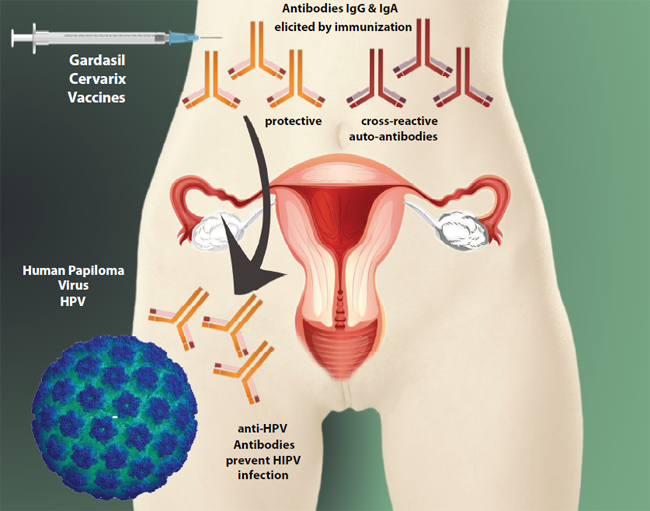
The quadrivalent vaccine Gardasil induces antibodies to prevent infection of either of 4 strains of HPV virus in the female genital tract. Effective antibodies must reach a sufficient concentration in body fluids to neutralize the virus during sexual intercourse with an infected partner. Multiple booster vaccinations are needed as well as an aluminum salt adjuvant to enhance the immune response. It is also important that antibodies solely attack the HPV L1 protein without mistakenly targeting endogenous tissues in vaccinated people (Kanduc, 2011). The ability of antibodies to recognize the right target is hard to predict since an accident called ‘molecular mimicry’ can induce antibodies capable of causing disease. We call these ‘cross-reacting’ antibodies or auto-antibodies (symbolized with carmine in the figure below). For example, both protective antibodies and cross-reacting antibodies are increased by adjuvants in disorders like ASIA syndrome due to the overall heightened immune response.
Antibodies and auto-antibodies are not theoretical or hypothetical constructs. They’re very real because Gardasil clinical studies fine-tuned the anti-HPV serum antibody concentrations by adding 2 booster vaccine doses plus an alum-based adjuvant, and God knows what else. Booster doses and adjuvant were considered necessary to awaken the immune response upon re-exposure and in fact, this is called the anamnestic response.
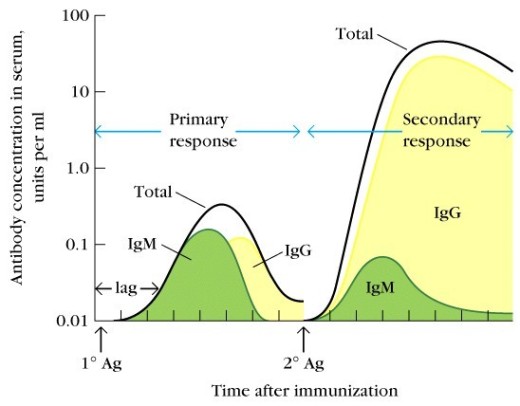
Primary and Secondary response. Figure 2 summarizes changes in antibody concentration in a new infection or vaccination. Initially, B lymphocytes produce Immunoglobulin M (IgM) that reaches high levels several weeks after infection or vaccination (primary response). When the booster dose of vaccine is administered (or there’s repeated infection), cells are reactivated and produce Immunoglobulin G and A (IgG & IgA) causing very high antibody concentrations (secondary response). Over time antibodies drop but can be readily reactivated with a booster dose or re-infection. One of the most important implications is that the auto-antibodies (cross-reacting antibodies) would do it likewise, and if harmful, their minor damage at the beginning will worsen with a reinforcement dose. As we shall see, this pattern fits perfectly with symptoms shown by our cohort of patients vaccinated with 2 or 3 doses of Gardasil.
(optional) Hypersensitivity type II mechanism. Diseases caused by auto-antibodies are abundant in Medicine. These are known as Hypersensitivities, type II and III are particularly relevant. Well known examples of type II hypersensitivity are Hashimoto’s thyroiditis, Graves disease and Goodpasture ‘s disease among others. To illustrate our discussion in terms of ‘molecular mimicry’ and immune-mediated mechanism are the neurological symptoms caused by antiglycolipid antibodies elicited by Campylobacter jejuni intestinal infection. Some susceptible individuals develop Guillain-Barré Syndrome. I mention Campylobacter infection because it educates us about antibody-mediated damage in a well-known disease to better understand the likely mechanisms of how the HPV vaccine could cause adverse events by molecular mimicry. Nerve demyelination produced by cross-reactive antibodies cause muscle weakness, numbness and neuropathic pain in relation to anti-glycolipid antibody titers. In many people the acute onset might lead to severe compromise of respiratory muscles and breathing requiring intubation. When antibody titers drop, so do symptoms and there’s a path to nerve regeneration and patient recovery (acute polyradiculoneuropathy). However, if antibodies rise again, the injury is repeated and symptoms return (chronic polyradiculoneuropathy). We call it a relapse or recurrence so typical of our patients vaccinated against HPV. Another mechanism of tissue damage is Type III hypersensitivity , also called immune complex disease because although it begins as a type II hypersensitivity, high levels of auto-antibodies bind to a large number of endogenous antigens to form macromolecular aggregates that deposit in the microcirculation of the kidney, joints and brain causing greater damage in neighboring tissues (innocent bystander). Within this framework we will summarize major findings results previously reported in detail in this blog.
Methods and patients.
This study is a survey of adverse events or symptoms that 62 young women developed after immunization against HPV. Their age was 14.5 years on average (+/- 2.1 standard deviation). Of these patients, 61 received the quadrivalent vaccine Gardasil in Colombia (55 from Carmen de Bolivar and 6 from other cities –Barranquilla, Bogota, Bucaramanga and Cartagena) and a girl received the bivalent vaccine Cervarix (Sonora, Mexico). This article summarizes findings reported but focuses on the overall pattern and relevant underlying mechanisms. Please notice that this blog is written in Spanish and links point to Hispanic language websites and references. Symptoms previously reported in greater detail are:
Because some patients might have unique manifestations that don’t fit the overall pattern their cases must be studied individually. This investigation was carried out completely with my own resources and counting on volunteer participation of subjects and parents. Thanks to all participants!. There are no conflicts of interest. For methodological details of this survey please click here, here and here. Symptoms to be analyzed in future installments are fainting or syncope as well as endocrine, gynecological, lympho-hematopoietic and cognitive/psychological symptoms. I’d appreciate victims to share with this author documentary evidence such as clinical tests, videos, photographs, physician diagnoses, and so on that help support and illustrate the impact of this disease. At the end, please read guidelines on how to collect these data.
Results and Discussion.
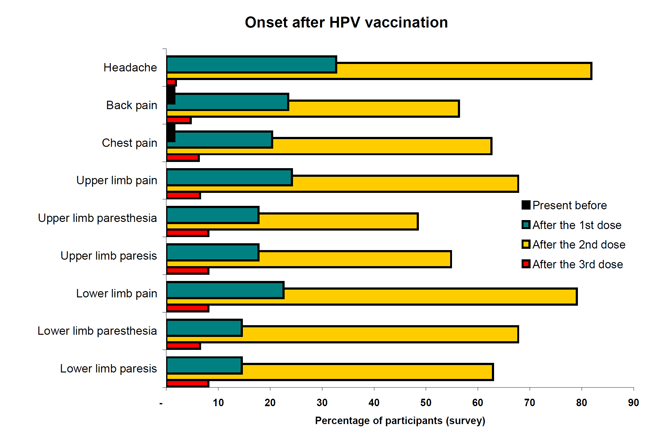
Temporal pattern of clinical manifestations. One of the strongest findings of this survey is the pattern of symptom onset after the first and second HPV vaccine dose (Figure 3). Such pattern applies to 3 pain syndromes (head, back and chest), and 6 neurological syndromes (paresis, paresthesia and dysesthesia) in upper and lower extremities. With the first vaccine dose only 15-30% of participants noted symptom onset; while 48-80% of girls said the symptoms appeared after the second dose. This cannot be a coincidence. This pattern completely agrees with the secondary antibody response or anamnestic humoral response triggered by the booster dose as described in Figure 2. It suggests that if auto-antibodies were elicited by the vaccine, symptom onset and disease severity go along with doses that cause greater antibody titers.
Interpretation: We can infer that auto-antibody concentration paralleled symptoms suffered by girls who became sick by Gardasil. That is, antibodies elicited by the first dose caused symptoms in a few girls; while greater antibody concentrations with a second dose would cause a greater number of them to fall sick. Although we have no lab evidence of antibodies changing in this fashion, we don’t need it, since it’s a well-established scientific fact that serum antibody titers increase with more vaccine doses. In fact, this evidence is replicated time and time again by scientists and pharmaceutical licensing studies like those of Gardasil and Cervarix.
To demonstrate an autoimmune basis in our patients we just need to find elevated auto-antibody titers pathogenically related to their disease. Alternatively we could uncover immune-mediated tissue damage in biopsy or postmortem studies if the opportunity arises. – But more relevant is evidence obtained on clinical grounds. For example, we know that if girls re-expose themselves to vaccine relevant antigens (some already present in their bodies), auto-antibodies rise thus explaining relapse. By contrast, removal of auto-antibodies should favor clinical improvement. Some girls have clinical records that support partial symptom remission with antibody removal therapies like IVIg and plasmapheresis. Positive response to antibody removal is evidence of humoral disease even if we fail to pinpoint specific antibodies. Still, girls might experience relapses due to residual inflammation or by traces of vaccine / adjuvant lodged in their bodies. A well known example is inflammation at the injection site called Macrophage Myofasciitis (deltoid muscle) but such inflammatory foci might be widely dispersed in lymphoid tissues throughout their bodies within macrophages and dendritic cells. So if a girl improves clinically after a granuloma is surgically removed from her shoulder, this is a strong proof that vaccine-related inflammation underlies her disease (please read Addenda 1 & 2 for a deeper discussion on the role of antibody titers, disease severity and improvement with antibody removal).
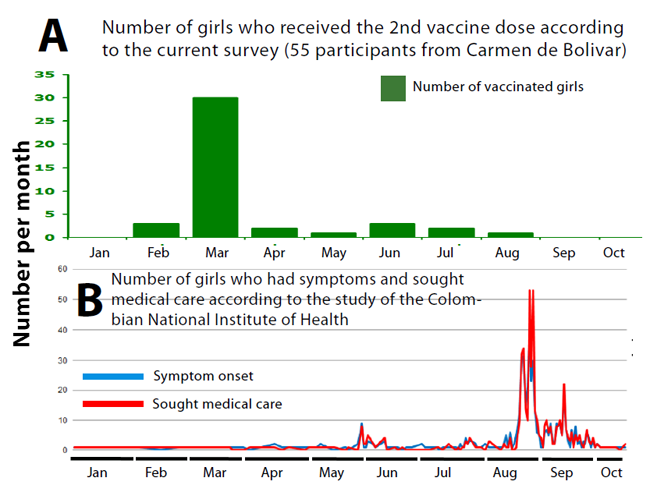
INS studies. Next, let’s turn to the symptom onset pattern reported by the Colombian National Institute of Health (INS). The INS didn’t publish or analyze the symptom onset after the first vaccine dose given during 2013. Possibly so few girls complained, their symptoms were mild or simply couldn’t track their origin. The INS data show only the symptom chronology after the 2nd dose application which occurred in 2014. To understand it, let’s first see Figure 4-A that depicts the number of girls/month who received the second dose of Gardasil in Carmen de Bolivar according to my survey. Please notice that most of them received it during March 2014, although 2-3 girls/month got the 2nd vaccine dose in other months. As expected from adverse events from vaccination symptoms should develop later. In fact, the INS report shows several peaks of patients experiencing symptoms and seeking medical care mostly in August-September/2014 (Figure 4-B). This pattern clearly shows that the appearance of symptoms occurred after vaccination by several weeks. Once girls developed symptoms, they immediately sought medical care as expected if they notice something going terribly wrong. As expected from autoimmune disease, it takes several weeks to make auto-antibodies, for these to cause organ damage and for people to seek medical care especially if symptoms appear slowly. In essence, the point of these graphs is to show that the INS symptom chronology is clearly associated with the second vaccine dose. And the reason symptoms stand out better with the 2nd dose is because they were more severe, affected a larger number of girls and had an epidemic pattern. Our data show that 2nd vaccine dose or first booster predated the epidemic appearance of symptoms just like the INS reported. There’s no disagreement on this point. Our interpretation is that if girls made harmful auto-antibodies with the first shot, greater antibody titers elicited by a second dose were more likely to cause disease.
Let’s go to Medellin to look at Valentina’s case (Colombia). Like many girls of her school, Valentina was forced to get the shot even if she refused because she experienced symptoms with the first one. The reinforcement dose for sure deepened injuries from the first shot. We know this from basic immunology and because if needed, such observations can be made prospectively in the about to-be-vaccinated girls and who are susceptible to the ASIA syndrome in Minister Gaviria’s indiscriminate vaccination campaigns. –

After these 2 doses of Gardasil, Valentina developed a number of symptoms to the point of being admitted to several hospitals where she has been in great danger. Hospitalization and life-threatening complications qualify as Serious Adverse Events. Please look at the following video where Valentina shows flaccid paralysis of at least 5 muscle groups in her body (not counting neck paralysis, she was quadriplegic). Lately her illness has improved but continues with ups and downs possibly related to cross-reacting antibody titers. To prove this, it’s just a matter of research but Health Minister Alejandro Gaviria would say no, because «the vaccine safety is close to 100%«.
@NataliaParis_ madre de 3 niñas víctimas de la vacuna del VPH No permitas a k tu hija mariana le hagan este mal😕 pic.twitter.com/LyASYOyXBe
— *:)mile:)* (@valentinov04) November 5, 2015
//platform.twitter.com/widgets.js
But Valentina’s parents didn’t buy Mr Gaviria’s political bullshit. Honestly, who would trust a non-physician politician making health recommendations?. – Well, Valentina’s parents decided to pay out of pocket a test for anti-glycolipid antibodies and shipped a blood sample to an USA lab. It came out with a not-so-surprising surprise: Valentina’s blood had high titers of auto-antibodies against nervous tissue damage, which is perfectly compatible with her symptoms of autoimmune neurological disease.

Cross-reacting antibodies underlie many autoimmune diseases, and oftentimes it’s possible to identify a trigger. Because only school age girls are the targets of Gardasil through the Expanded Immunization Program, it makes perfect sense that the HPV vaccine is the common trigger that explains neurological demyelinating disorders like the ones described here and that appear in Gardasil’s Adverse Event profile (see page 12). Additionally, anti-glycolipid antibodies like those found in Valentina’s blood cause demyelinating diseases observed in mass flu vaccinations (Nachamkin et al, 2008). In addition, the Gardasil vaccine is particularly suspicious because it contains an aluminum-based adjuvant that enhances immune responses including those potentially harmful to the organism.
The therapies that have helped Valentina survive are those that eliminate or interfere with harmful auto-antibodies. Her medical history supports multiple sessions of plasmapheresis to clear auto-antibodies from her blood and anti-inflammatory corticosteroid drugs that have caused Cushing syndrome. Her medical records also show that Intravenous Immunoglobulin G (IVIg) has been administered multiple times, with the purpose to dilute cross-reacting antibodies ( ‘dilute the bad with the good’). In her last hospitalization Valentina could not walk and had nosebleeds probably due to autoimmune vasculitis. Upon receiving IVIg her symptoms improved but relapses often require additional IVIg applications.
Valentina’s suffering has contributed to our knowledge and makes us wonder if a disease like hers also affects the more than 700 girls in the country. The answer to this question depends on carrying out a transparent, medical and scientific investigation that the Health Ministry and affiliated agencies have hampered so far. Below we summarize extra findings gathered in the symptom survey. For a discussion on how symptoms correlate with antibody titers in autoimmune disease please read Addendum 1 at the bottom of this article. For a discussion on how plasmapheresis is recognized as first line therapy to certain autoimmune neurological diseases, please read Addendum 2. Both of these arguments and documentary evidence support that elevated anti-glycolipid antibodies in Valentina’s blood as well as the favorable response to plasmapheresis and IVIg are extremely strong pieces of evidence for autoimmune neurological disease associated with HPV vaccination.
Headache
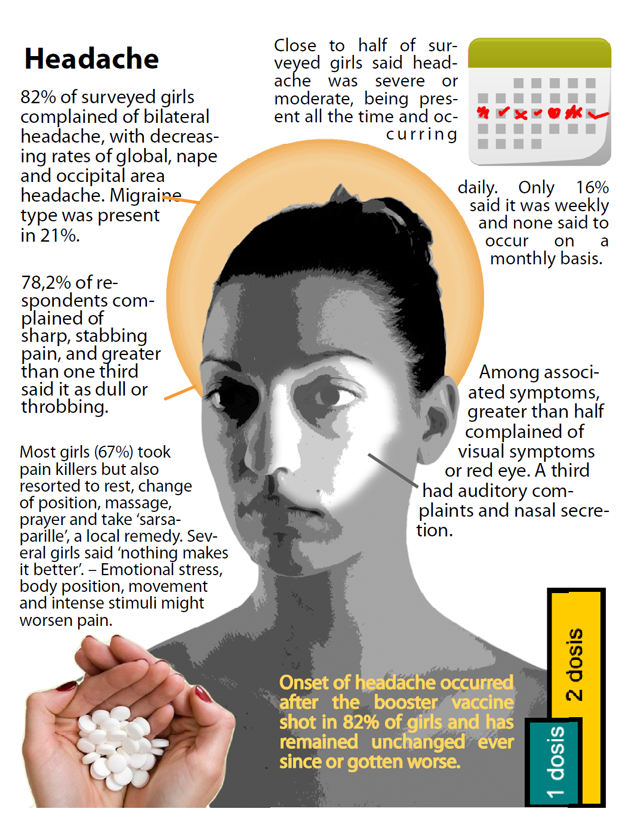
Headache was the universal symptom experienced by 100% of the 62 surveyed girls. It was experienced as a global headache, with stabbing, throbbing but also dull characteristics. Some respondents reported that pain was associated with red eye, runny nose, visual and auditory symptoms. It was rated severe or moderate; of constant or daily frequency. It has some features of migraine, tension and cluster headaches without being typical of any one in particular. – In a third of respondents, the headache started after the first dose of Gardasil but the vast majority experienced after the second HPV vaccine dose. The same proportion said that headache hasn’t improved and a quarter said it’s become worse. Stress, body position, movement and sunlight can worsen the pain. To relieve it, girls take painkillers, rest, position changes, massage, prayer and folk remedies like sarsaparilla. Some participants said ‘nothing relieves it’. A few girls have attempted suicide, one suceeded.
Headaches appeared mainly after the booster dose of Gardasil suggesting auto-antibody-initiated mechanisms. Due to the proximity of cephalic structures to where the shot was given in the shoulder, suspicion is raised of whether nociceptive or neuropathic mechanisms are at play. Both would qualify as both are triggered by inflammation. It’s important to remember that the HPV vaccine is par excellence a synthetic and biological product of inflammatory nature, designed to stimulate the Innate Immune Response via the aluminum adjuvant and the Adaptive Immune Response through the HPV L1 recombinant protein antigens. Both of these mechanisms trigger advanced stages of inflammation by recruiting phagocytes, antigen presenting cells, T and B cells and cytokines whose manifestations make this symptom relevant. In severe cases like those associated with cerebral vasculitis can cause death (Tomljenovic & Shaw, 2012). For example, these authors report cerebral vasculitis in 10.9% of 2,385 cases of headache and migraine in vaccinated women with Gardasil and Cervarix according to reports to the VAERS database 2006-2012. A staggering statistic.
Similar to the severe headache reported here, Dr. Louise Brinth in Denmark found that headaches affected all the 53 girls vaccinated with Gardasil who participated in her study.
Despite Dr. Brinth’s efforts to warn about the harmful adverse event profile of Gardasil on Dannish girls (~Sep 2013), the Colombian Ministry of Health was full blast with the HPV immunization campaign. It’s hard to believe that despite living in a globalized world with instant communications thanks to fiber optic technology capable of crosssing oceans at the speed of light, and that despite Europe, Japan and the United States have joined efforts to standardize the ethical handling of drug development through the ICH –International Convention of Harmonization and now followed by all countries, despite that, warnings from Denmark were systematically ignored. So when the PAI – Extended Immunization Plan in Colombia targeted school age girls, there was nothing to protect them from the disastrous effects of Gardasil vaccine being repeatedly announced in Denmark. Later, we came to find out that Colombian National Institutes of Health outbreak report informs that 517 girl histories qualified as genuine cases of sudden symptom onset after vaccination with Gardasil. From this cohort, 414 girls (80.1%) had headache and other abnormal symptoms. Surprisingly, like a prestidigitator this non-peer reviewed study magically concludes that vaccination with Gardasil despite being the only common factor among affected girls is unrelated to their disease. But the effrontery doesn’t end there. The medical and scientific staff of the Colombian Ministry of Health and the National Institute of Health forgot that 517 girls were suffering and needed treatment. After more than a year of their report, the Health Minister Alejandro Gaviria insists that patients do not suffer, nor do they deserve a diagnosis and treatment. He even threatens those who think otherwise (read the rest of this story in Addendum 3 at the bottom of this article).
Let’s return to symptoms shown by 62 surveyed patients who received 2 or 3 doses of the HPV vaccine.
Chest pain
Ninety one percent (91%) of respondents experienced precordial pain of stabbing, oppressive, constant or throbbing nature. It was constant or occurred daily. Half of participants considered it very intense and a quarter considered it moderate. Drugs, rest, position changes, exercise, massage and prayer were measures used to alleviate it. Factors that made it worse were activity; position changes and ‘crises’ described as syncope that can evolve into seizures. Chest pain started with the first and second dose of the HPV vaccine and generally stayed unaltered or has worsened. A majority of participants expressed difficulty breathing (dyspnea, asphyxia, shortness of breath) associated with chest pain, along with nausea, palpitations, tingling and fainting – syncope. Similarly high incidence statistics were reported by the Colombian National Institute of Health: 246 girls (41.8%) suffered chest pain, 148 (28.6%) suffered dizziness / vertigo, 125 (24.2%) suffered syncope, 105 (20.3%) experienced shortness of breath (see table 11 of the INS outbreak report).
The following video illustrates a ‘crisis’ that Camila suffers. Typically it starts with chest pain, shortness of breath, nausea, palpitations, fainting, and seizures in some girls.
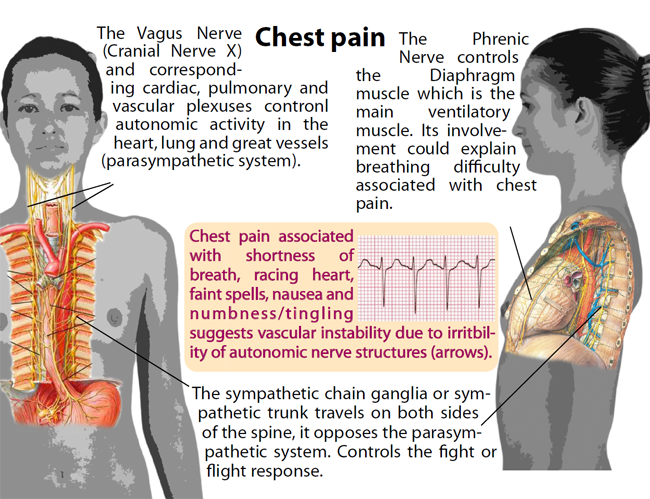
To understand this we need to review at least 3 main structures.
- The Vagus Nerve (Cranial Nerve X) that runs through the thorax and gives off corresponding cardiac, pulmonary and vascular plexuses which control autonomic functions of the heart, lungs and great vessels through an extensive network of nerve endings (parasympathetic system).
- The chain of sympathetic ganglia or a.k.a. sympathetic trunk runs attached to both sides of the spine and controls the fight-or-flight response, or those functions opposite to the parasympathetic system.
- The Phrenic nerve controls the diaphragm muscle which is the main ventilatory muscle. –
Under the scenario of the neuropathic hypothesis, antibody-mediated demyelination can damage these nerve structures making them irritable and likely to trigger difficulty breathing, nausea, palpitations and ultimately fainting or syncope. Patients have clearly associated chest pain to these symptoms. It’s worth mentioning that Dr. Brinth in Denmark found that 66% of her case series (53 girls) complained of chest tightness or actual pain associated with shortness of breath. Her conclusions read textually «the pathogenic alteration is located in the autonomic nervous system«. Therefore, it would be desirable to document dysautonomic damage through a specialized approach just like Dr Brinth did in Denmark.
Depending on symptom frequency, evaluation of dysautonomic syncope should be approached this way:
- If fainting or near-fainting happens once a month or week, it is advisable to use a portable ‘Cardiac Event Recorder’ that the child can activate it as soon she experiences dizziness or palpitations before fainting.
- Alternatively, a portable 24-hour Holter monitoring also records heart activity and blood pressure. Patient Maria Jose was initially identified with dysautonomic syncope by this test.
- If blackouts, lightheadedness or fainting are frequent (several times per week) or manifest themselves by getting up from bed or chair (orthostatism); a Head up Tilt Table Testing should be done. This test was also positive for patient Maria José. It’s possible that in the course of disease this test may be interpreted as POTS (Postural Orthostatic Tachycardia Syndrome) which suggests systemic sympathetic over-compensation.
- If previous attempts to record cardiac activity fail, cell phone adapters can be used by family to get some tracings for later evaluation by a cardiologist.
To support an autoimmune basis of chest pain and associated symptoms, auto-antibodies against autonomic structures should be sought. We suspect demyelination of nerve endings in cardiac, pulmonary or vascular plexuses. I don’t think involving yourself into a personal journey of biomedical research is justified since medical care should be provided just based on patient complaints. However, we’ve seen that doctors and health authorities in developed countries stonewall patients’ efforts to find explanations for this epidemic of symptoms in girls vaccinated with Gardasil. – Particularly helpful has been Dr. Svetlana Blitshteyn’s efforts. She has studied vaccinated girls with Gardasil who developed POTS Syndrome and dysautonomia. In a larger case series, certain auto-antibodies correlate with dysautonomic disease. In cited studies, there’s evidence of higher prevalence of antinuclear antibodies (ANA), anti-phospholipid antibodies (aPL), antibodies against ganglionic type N acetylcholine receptor, beta1- and beta-2 adrenergic receptors, and antibodies against M2- and M3 Muscarinic Receptor. These tests should be included among more comprehensive immunological panels.
Upper limb neurological symptoms
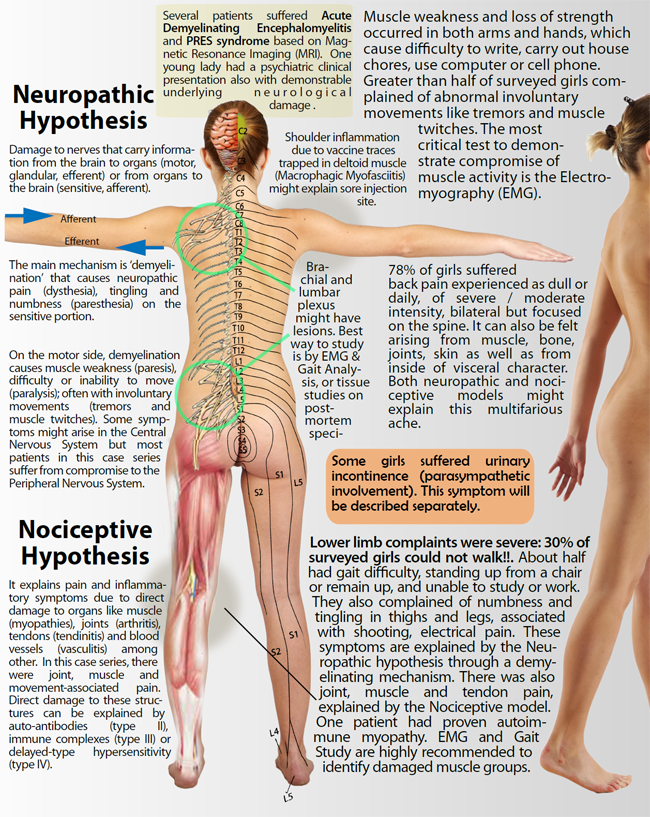
Sensitive branch: Sensation loss was characterized by tingling and numbness of both hands and arms that began after the second dose of Gardasil and has not improved since then in most vaccinated girls. Upper extremity pain in 62 respondents was very intense, paroxysmal-electric (shooting) character that affects hands and arms bilaterally, which tends to worsen with activity, position or cold but relieved by similar maneuvers and changes in position, rest, exercise or medication. 43% of girls complained of pain at the injection site in the shoulder.
Motor branch: Weakness and loss of muscle strength affected both arms and hands, making it difficult to write, perform household duties, and using computer or cell phone. More than half of respondents reported abnormal involuntary movements of the arm such as tremors and muscle twitching (fasciculations).
Please observe the following video of a teenager vaccinated with Gardasil where fine spontaneous muscle twitches of the ‘fasciculation’ type can be seen. These low amplitude tremors are signs of ‘denervation’ and in this young lady’s hand, they involve the Interosseous and Lumbrical muscles. Electromyography (EMG) can confirm electrically what we see with our eyes. It is impossible that a twitching muscle returns a ‘normal’ EMG.
Hand fasciculation video here.
To workup these complaints, I recommend Electromyography (EMG) of affected muscles, as it can record involuntary muscle movements plus other like fibrillations imperceptible to the human eye. Each muscle is punctured with a needle-shaped electrode that records twitches and fibrillation electrical activity . – Conversely, if an affected girl suffers twitches but her EMG is reported as ‘normal’, that reading should be questioned. Another test is the Nerve Conduction Velocity (NCV) also known as Nerve Conduction Studies (NCS) that is only informative if it comes out as ‘low speed’ in the context of a peripheral demyelinating neuropathy that affects the nerve along its length. But if it’s normal, then damage at roots and plexuses should be suspected. Because of the difficulty of measuring conduction speed in nerve roots and plexuses in their exit from the spine, it’s advisable to perform EMG instead of VCN. In selected patients, myopathy should be ruled out by serum muscle enzymes (creatine Phosphokinase -CPK, aldolase and myoglobin) as well as rheumatological disease antibodies. –
Back pain
Back pain was experienced by 78% of patients and reported as constant or daily; of moderate or severe intensity. Its location was in the spine with irradiation to both sides and is experienced as muscle, bone, joint, skin but also felt as deep and visceral. It can be explained by both neuropathic and nociceptive hypotheses. There was also cervical neck and pain of the same characteristics.
Body position and activity worsened pain but other factors such as ‘crises’ and stress at school were associated too. Medicines, exercise, position changes, massage and prayer were used to relieve pain. It began after the first and second dose of the HPV vaccine and has been unchanged since. Associated symptoms were difficulty moving or walking, electrical shooting ‘sciatica’ pain and interference with sleep. In this regard, it’s likely that some patients suffer from fibromyalgia although physical examination is required for confirmation. In a symptom survey of 45 patients from 13 countries, Dr Manuel Martinez-Lavin et al (2015) inquired for fibromyalgia symptoms accepted by the American College of Rheumatology and found that 53% of participants fulfilled criteria for this diagnosis. Since some patients in our cohort also filled out surveys in Dr. Martinez-Lavin study, they could potentially receive the same diagnosis.
Dr. Juan Manuel Anaya et al (2015) described 3 Colombian teens who suffered joint symptoms after Gardasil vaccination. After an extensive battery of tests, it was found that one patient had systemic lupus erythematosus, another had rheumatoid arthritis and another suffered a spine disease called spondyloarthropathy. These cases support direct damage to organs other than the nervous system or the nociceptive hypothesis. However, most victims of HPV vaccine suffer from neuropathic pain due to damage to nerve structures.
Lower limb neurological symptoms
Sensitive branch. Pain affected the entire length of both lower limbs, sciatica was intense and moderate also experienced as muscle soreness. It was constant or daily, associated with weakness and difficulty walking. Also, there were joint pain in knees, hips and ankles. The pain got worse with activity, cold, stance and prompted victims to seek relief through medication, rest, position change or even exercise. Pain began with the first and second HPV vaccine shot, has worsened in a quarter of girls and remained unchanged in half of the respondents. In addition, patients complained of tingling and numbness in both legs and thighs and shooting pain or ‘sciatica’. No patient suffered loss of sensation before vaccination and its onset occurred after ‘booster’ dose of Gardasil. Half of the patients still complain of such symptoms and a quarter said it’s gotten worse. In S-LANSS pain survey done on 19 participants from Carmen de Bolivar, we found that the pain was severe and of neuropathic origin.
Motor branch. Most survey respondents expressed weakness and loss of muscle strength that compromised gait in greater than 70% of girls. Specific manifestations were difficulty walking, standing up from a chair, and simply maintaining the up stance. But the most devastating complaint was inability to walk in a third of the participants!!. Tremors and muscle twitches accompanied muscle weakness. Clinically, this pattern is interpreted as ‘denervation’. Symptoms became apparent after the second dose of Gardasil.
These surveys suggest damage to the peripheral nervous system by evaluation of 2 sensitive branch symptoms: neuropathic pain (dysesthesia) and loss of sensation (paresthesia) and 1 motor branch (muscle weakness and abnormal movements). This matches a lower motor neuron syndrome that could exhibit hyporeflexia and hypotonia in physical examination. We can’t rule out nociceptive damage in some participants who complained of muscle pain and arthralgia, but the bulk of victims seem to suffer from demyelination to peripheral nerves. A lesion is harder to locate if Nerve Conduction Studies come back normal and we should suspect injury to nerve roots and lumbar plexus (or brachialis plexus for upper limb disease) as they exit the spine. Documenting injuries at these levels can be challenging and thus EMG and gait analysis (walking gait analysis or assessment) can help focus on affected muscle groups. The extent of the muscle weakness can be estimated through dynamometers designed for that purpose, especially if improvements during therapy are being followed up.
To illustrate these issues, let’s look at a video of a teenager from Carmen de Bolivar who walks with great difficulty after HPV vaccination. We should ask what the Observational Gait Analysis diagnosis would be after a Rehabilitation Medicine specialist evaluates her gait.
Espiritu Santo Video girl here.
In order to demonstrate injury to lumbar nerve roots and plexus as they exit the spine (or brachial plexus in case of upper limbs), a biopsy or autopsy would yield data of gold standard quality. However, biopsy is invasive and not recommended; rather it’s better to wait for post-mortem studies if a child dies. We are aware of 3 girls who died in Colombia and one of Mexico after becoming sick upon HPV vaccination, we still don’t know if their tissues were investigated. Although it’s painful to talk about death, one of the most revealing studies was carried out by Lucija Tomljenovic & Christopher Shaw in 2 girls who died of cerebral vasculitis after HPV vaccination.
The Colombian National Institute of Health (INS) reported that a total of 517 girls developed symptoms after vaccination, 312 (60.4%) had lower limb paresthesia, 239 (46.2%) had upper limb paresthesia, 78 (15.1%) reported muscle weakness, 49 (9.5%) had perioral paresthesia, 31 (6%) had joint pain and 11 (2.3%) had twitches. Despite methodological differences with the present blog report, the high incidence of neurological adverse events reported by INS suggests an association to vaccination with Gardasil. That is, there is no denying that victims experienced these symptoms after HPV immunization so they qualify as authentic Adverse Events to be informed in Phase 4 studies or Post-licensing (Surveillance) studies. In other words, it’s time to start using the appropriate language and research methods. The few workup studies done in a few participants suggest specific mechanisms of tissue damage triggered by the vaccine. It’s still possible to do more and better but the Ministry of Health has hampered research and has abandoned victims forcing them to sue the State and summon legal resources to defend their rights. It is curious that the “Ley Estatutaria’ recently signed and approved by Minister Gaviria to declare health as a Colombian right, has in Mr. Gaviria himself the first violator.
Conclusions
In this issue I summarize complaints of headaches, chest and back pain as well as motor and sensory symptoms of upper and lower limbs. The predominant group of symptoms point to a demyelinating autoimmune disorder triggered by immunization with the quadrivalent Gardasil and bivalent Cervarix vaccine (in one patient) and their lot specific components. We discuss mechanisms that might underlie many of these symptoms and suggest some tests that could help victims better document their disease. We cannot rule out the presence of genetic or environmental susceptibilities in the cluster of Carmen de Bolivar, Colombia. – Because there are susceptible individuals in every population, we must exercise the century-old medical principle «primum non nocere» or more modernly, «assess before vaccinating«. We should also ask for informed consent to spare unnecessary disability in people with recognized immunological derangements. Massive and indiscriminate immunizations should be avoided because no medical or health intervention is 100% effective and we expect a small percentage of people who might be unnecessarily subjected to pain and suffering. Additionally, we should stop defending a yet unproven risk-benefit balance that justifies ‘a small number of victims’. HPV vaccination has not saved a single life while it has already endangered many of innocent girls and women (there are also men some who have emailed me). Studies show that the vaccine is particularly effective to reduce infections of 4 strains of the HPV virus but we know that 70% of people spontaneously eliminate them without vaccination. We still don’t know if current dosing schedules maintain effectiveness for the 20-30 years a tumor might take to settle and grow. During that time it’s possible to identify and eliminate carcinoma in situ through regular gynecological Pap smear surveillance (Vaginal Cytology – Papanicolau). Most likely, Gardasil and Cervarix promises of reducing cancer rates may turn out a macabre and tasteless joke.

Diagnostic impression
We have the diagnostic impression of an autoimmune neurological disease mediated by auto-antibodies in 62 participants of this survey. However, each patient should be evaluated individually because her symptoms may differ from the general pattern reported here. Therefore I recommend to rule out the following diagnoses and pathologies:
- Demyelinating polyradiculoneuropathy (acute or chronic)
- Guillain-Barré syndrome
- Demyelinating Encephalomyelitis (acute or chronic)
- PRES syndrome
- Transverse myelitis
- ASIA syndrome
- HANS syndrome
- Fibromyalgia vs. Chronic Fatigue Syndrome
- Autoimmune myopathy
- Macrophagic Miofasciitis (of the shoulder)
- Autoimmune arthropathy
- Dysautonomia – Sympathetic, Parasympathetic
- Syncope: Dysautonomic vs. Neurocardiogenic
- POTS syndrome
- Complex Regional Pain Syndrome II / Causalgia / Reflex Sympathetic Dystrophy
- Immune complexes disease (e.g., vasculitis, lupus, anti-phospholipid syndrome among others)
- Secondary complications (renal failure, disability labor school, secondary cognitive and psychological disorders among many others impossible to list here).
Recommendations
The presumed mechanism of injury triggered by HPV vaccination is generation of auto-antibodies or cross-reacting antibodies. Because health authorities are dragging their feet, parents need to take an active role to secure an accurate diagnosis. In addition to other minor suggestions, the most important recommendation is to collect serum when the disease is most active (flare ups) and while the girl is not receiving or have not recently received anti-inflammatory treatments such as corticosteroids or anti-neoplastic chemotherapy, or procedures to remove antibodies such as IVIg and plasmapheresis.
- The blood sample must be collected (10 mL) and allowed to clot or coagulate (red cap tube)
- Centrifuge
- Serum should be separated within 30 minutes into sterile plastic vials labeled with patient’s name
- Freeze serum vials at deep cold (-20 degrees Celsius or colder) and keep them until shipment which may be done several weeks or months later.
- Initial processing of the blood sample can be done in any clinical laboratory of any urban neighborhood (all steps above).
- When a neuromuscular specialized laboratory is found and arrangements are made, the sample can be shipped to analyze auto-antibodies and anti-glycolipid antibodies (3-5 mL of serum is needed).
- Transit time should not exceed 48 hours and if so the sample can be shipped defrosted (at room temperature).
- Auto-antibodies to investigate should not be limited to those mentioned here and generally should focus on group of disorders like those causing demyelinating, autonomic, sensory and motor damage to the nervous or neuromuscular systems. Rheumatological tests can be run at the same time.
‘Chelation therapy’ should be avoided as it has no role in managing autoimmune diseases. If patients were told that heavy metal chelation therapy led to their recovery, they should be suspicious that it might have been a façade to provide IVIg or other form of anti-inflammatory therapy. Patients should seek legal advice to subpoena clinical records and find out what was really done. The vaccine itself contains aluminum as amorphous crystals that are deposited within phagocytic cells and that are impossible to remove by chelation. Chelation is an invasive, risky procedure and has no place in the management of autoimmune disease. It should be avoided.
Acknowledgements
To girls, teens and adult patients who voluntarily provided information about their illness. Thanks to moms and parents who consented to this survey study. Thanks to community leaders in Carmen de Bolivar Blanca Victoria Sabagh representative of the NGO “Organization for the Defense of Citizens’ Rights or ODDC” , Candelaria Montes Romero, Hector Miranda, Zamira Peñaloza. Special thanks to Maria Rivera who manually tabulated anonymized surveys and has been a champion of this cause. Thanks to all ‘the cute little warriors’. Special thanks to journalist Mario Lamo and the «Rebuilding Hope Association» (Asociación Reconstruyendo Esperanzas) for their outreach and indefatigable documentation of cases through videos, photographs and testimonies that have helped mobilize efforts to advance justice and health for these innocent victims. – Please forgive if I don’t mention the names of so many people whose national and international communications have contributed to and have helped me understand this disease. Many families have sent pieces of their daugthers’ clinical histories but because of data fragmentation I have been unable to put their valuable testimonies together. It’s also due to my lack of time (mea culpa). To all of you thanks a million!.
Bibliography
- Brinth LS, Pors K, Theibel AC, Mehlsen J. (2015). Orthostatic intolerance and postural tachycardia syndrome as suspected adverse effects of vaccination against human papilloma virus. Vaccine. May 21;33(22):2602-5
- Blitshteyn S (2014) Postural tachycardia syndrome following human papillomavirus vaccination. Eur J Neurol.;21(1):135-9.
- Blitshteyn S (2015) Autoimmune markers and autoimmune disorders in patients with postural tachycardia syndrome (POTS). Lupus. 2015 Nov;24(13):1364-9.
- Martínez-Lavín M, Martínez-Martínez LA, Reyes-Loyola P. (2015). HPV vaccination syndrome. A questionnaire-based study. Clin Rheumatol. 2015 Nov;34(11):1981-3.
- Anaya JM, Reyes B, Perdomo-Arciniegas AM, Camacho-Rodríguez B, Rojas-Villarraga A. (2015). Autoimmune/auto-inflammatory syndrome induced by adjuvants (ASIA) after quadrivalent human papillomavirus vaccination in Colombians: a call for personalised medicine. Clin Exp Rheumatol. Jul-Aug;33(4):545-8.
- Martínez-Lavín M (2014). Fibromyalgia-like illness in 2 girls after human papillomavirus vaccination. J Clin Rheumatol. Oct;20(7):392-3
- Martínez-Lavín M. (2015). Hypothesis: Human papillomavirus vaccination syndrome–small fiber neuropathy and dysautonomia could be its underlying pathogenesis. Clin Rheumatol. 2015 Jul;34(7):1165-9. doi: 10.1007/s10067-015-2969-z. Epub 2015 May 20.
- Nachamkin I, Shadomy SV, Moran AP, Cox N, Fitzgerald C, Ung H, Corcoran AT, Iskander JK, Schonberger LB, Chen RT. (2008). Anti-ganglioside antibody induction by swine (A/NJ/1976/H1N1) and other influenza vaccines: insights into vaccine-associated Guillain-Barré syndrome. J Infect Dis. Jul 15;198(2):226-33. doi: 10.1086/589624.
- Kinoshita T, Abe RT, Hineno A, Tsunekawa K, Nakane S, Ikeda S. (2014). Peripheral sympathetic nerve dysfunction in adolescent Japanese girls following immunization with the human papillomavirus vaccine. Intern Med.;53(19):2185-200.
Addendum 1.
Antibody titers and clinical symptoms. The medical literature supports that antibody titers and clinical course are related thus lending credence to the relationship among vaccine doses, antibody titers and adverse clinical outcomes.
For example Ohguro et al (1993) studied patients with Multiple Sclerosis (MS), an autoimmune disease of the Central Nervous System, and found that anti-arrestin auto-antibodies correlated with disease activity being higher during exacerbation and lower during symptom remission.
Similarly, Hohlfeld et al (1985) studied 15 patients with Myasthenia gravis, an autoimmune neuromuscular disease, and found that titers for Anti-Acetylcholine Receptor antibodies closely correlated with clinical course, increasing in patients with relapses but not those in clinical remission.
Dupuy et al (2004) studied 3 patients with refractory pemphigus vulgaris, an autoimmune skin disorder, and found that treatment with Rituximab improved clinical symptoms with dropping anti-epidermis antibodies.
In an independent study Ahmed et al (2006) found that rituximab therapy against pemphigus vulgaris caused a sustained decrease in antikeratinocyte IgG4 antibodies that correlated with disease activity.
Possibly more reassuring is the study done by Thai et al (2014) that evaluated 126 patients with Wegener’s disease (Granulomatosis with polyangiitis) and PR3-ANCA antibodies were measured by Indirect Immunofluorescence and ELISA. The authors found that in 60% of patients there was a close correlation between ANCA-titer changes and clinical outcomes, in other words, that ANCA were always positive during relapses and negative during remission.
These studies in various autoimmune disorders support that antibody titers correlate with disease activity and have clinical and pathophysiological significance. Of course, there are exceptions. Some studies don’t find such correlation especially in advanced diseases whose well entrenched cell-mediated mechanisms have gone beyond whatever initial damage antibodies might have caused.
NOTES
Ohguro H, Chiba S, Igarashi Y, Matsumoto H, Akino T, Palczewski K. (1993). Beta-arrestin and arrestin are recognized by autoantibodies in sera from multiple sclerosis patients. Proc Natl Acad Sci U S A. Apr 15;90(8):3241-5.
Hohlfeld R, Toyka KV, Besinger UA, Gerhold B, Heininger K. (1985) Myasthenia gravis: reactivation of clinical disease and of autoimmune factors after discontinuation of long-term azathioprine. Ann Neurol. Mar;17(3):238-42.
Dupuy A, Viguier M, Bédane C, Cordoliani F, Blaise S, Aucouturier F, Bonnetblanc JM, Morel P, Dubertret L, Bachelez H. (2004) Treatment of refractory pemphigus vulgaris with rituximab (anti-CD20 monoclonal antibody). Arch Dermatol. Jan;140(1):91-6.
Ahmed AR, Spigelman Z, Cavacini LA, Posner MR. (2006). Treatment of pemphigus vulgaris with rituximab and intravenous immune globulin. N Engl J Med. Oct 26;355(17):1772-9.
Thai LH, Charles P, Resche-Rigon M, Desseaux K, Guillevin L. (2014) Are anti-proteinase-3 ANCA a useful marker of granulomatosis with polyangiitis (Wegener’s) relapses? Results of a retrospective study on 126 patients. Autoimmun Rev. Mar;13(3):313-8.
Addedum 2.
Possibly more definitive is the relationship between auto-antibody removal and clinical improvement. In this regard, the gold standard procedure is plasmapheresis. Cortese and Cornblath (2013) reviewed the role of total plasma exchange (plasmapheresis) in neurological disease as judged by three main scientific bodies: The American Society for Apheresis (ASFA), the American Academy of Neurology and the Cochrane collaboration.
This review concludes that plasmapheresis is considered first line therapy, either as a primary stand-alone treatment or in conjunction with other modes of treatment in diseases like chronic inflammatory demyelinating polyradiculoneuropathy (CIDP), Guillain-Barré syndrome (GBS), myasthenia gravis (MG) (moderate-severe), MG (pre-thymectomy), paraproteinemic polyneuropathies (IgG/IgA), paraproteinemic polyneuropathies (IgM), and pediatric autoimmune neuropsychiatric disorders associated with streptoccal infections (PANDAS) and Sydenham’s chorea. Even though plasmapheresis might be useful as second line therapy in other disorders, for the purpose of this article suffice it to say that harmful antibody removal through plasmapheresis is standard of care in some immune mediated neurological diseases and the favorable response is an independent proof for the role of antibodies in these diseases.
NOTES
Cortese I, Cornblath DR. (2013) Therapeutic plasma exchange in neurology: 2012. J Clin Apher. 2013 Feb;28(1):16-9. doi: 10.1002/jca.21266.
Addedum 3.
For international readers, it’s important to provide some background. The then Colombian National Institute of Health (INS) director, Dr. Fernando de la Hoz led the study that will be remembered in the annals of Colombian medicine as the first physician and epidemiologist to describe the first and only cases of post-vaccine massive psychogenic disease. Even though there has been no follow-up, prognosis, biological marker identification or control of risk factors of this rather bullshit diagnosis, he continues educating physicians at the Faculty of Medicine in the National University in Colombia.
But we can go deeper. Prior to that, Dr. De la Hoz had done an epidemiological study on Hepatitis B vaccination in the Colombian Amazon to qualify for his Ph.D. degree at the London School of Hygiene and Tropical Medicine. Even though the Hepatitis B immunization campaign targeted indigenous ethnic groups not accultured to the mainstream of Colombian society, he did not observe a single case of massive psychogenic disease. Yet when he studied teenagers in Carmen de Bolivar fully entrained to the mainstream Colombian society just like elsewhere in the country, he found an outbreat of only adolescent girls targeted by Extended Program of Immunizations –PAI. He still diagnosed massive psychogenic disease. – Soon after (January 2015), Dr. Fernando de la Hoz resigned from this post as director of Colombian National Institute of Health. But for the sake of story telling, this epidemic has many twists and turns. Months prior, Dr. Ivan Mendoza, an electrophysiologist in Florida, USA made the same diagnosis without hiring a single employee, or carrying out a single study, or even bothering to visit the semirural population in the Colombian Atlantic Coast. Possibly he just made a phone call to Mr Alejandro Gaviria who later texted his message in Twitter. Dr. Mendoza ingenuity deserves admiration because he diagnosed a rather unique unknown disease called massive psychogenic syncope (ICD code?) without even running a single electrocardiogram as his medical specialty requires. In short, hats off to this physician, ‘an Illuminati’ for sure. – But among the three, if we were to compare De la Hoz, Mendoza and Gaviria, certainly the non-physician and Health Minister Alejandro Gaviria is the wildest of all 3, his audacity has no limits: in his Twitter account he has threatened to prosecute those who think the HPV vaccine is to blame. For sure, they all belong to the same conspiracy.
(Translation of Mr. Gaviria’s twitter = We don’t rule out legal action against those who undermine trust in our vaccination programs with false accusations).

Reblogueó esto en RI against HPV mandate #NOHPVmandateRIy comentado:
Lengthy post. #NOHPVmandateRI
Reblogueó esto en lifebiomedguruy comentado:
What have we done unleashing this on people.